Month: April 2015
Why the Direct Pay Model would work well for the poor population.
One of the ideas which people perceive about Direct Primary Care is it’s only affordable for wealthier incomes. This article, which was well written by Marguerite Duane, MD, MHA, debunks the reasoning behind it. The link to the original article can be found at the bottom of the page.
So, if poor people have little to spend, why would the direct primary care model work for them? Simple; with direct pay models the actual health care costs can be kept much lower and therefore more affordable for these very patients. Plus, since direct pay models often have smaller patient panels, these patients may have more time with their physicians and staff to address the myriad of issues in their life that may be affecting their health.
Some direct pay models charge patients a monthly or yearly membership fee that covers all primary care office visits and even some basic or in-house labs. For example, at Qliance in Seattle, depending on the patients’ age, members pay a fee that ranges between $54 – $94 a month, which includes:
- 7 -day a week access to the Qliance health care team
- Same or next-day appointments for urgent care
- 30-60 minute office visits
- Phone appointments and e-visits
- After hour phone access to a physician for urgent medical needs
Sure, direct primary care is great because it covers all primary care visits, but you may wonder how will poor patients pay for labs or specialty visits? It may surprise you to learn that the actual cost of most basic labs is actually very little. We negotiated with local labs to pay just above the actual cost of the tests and in exchange, we pay our lab bill in full monthly. Here is an example of how it would work for a patient with diabetes:
Labs Actual Cost Patient Paid at time of visit
- HgAIC $8.72 $10
- Lipid panel $3.47 $ 5
- CMP $4.21 $ 5
What about the cost of specialty care, clearly this is much too expensive for poor people to afford, right? My response to that question is two-fold:
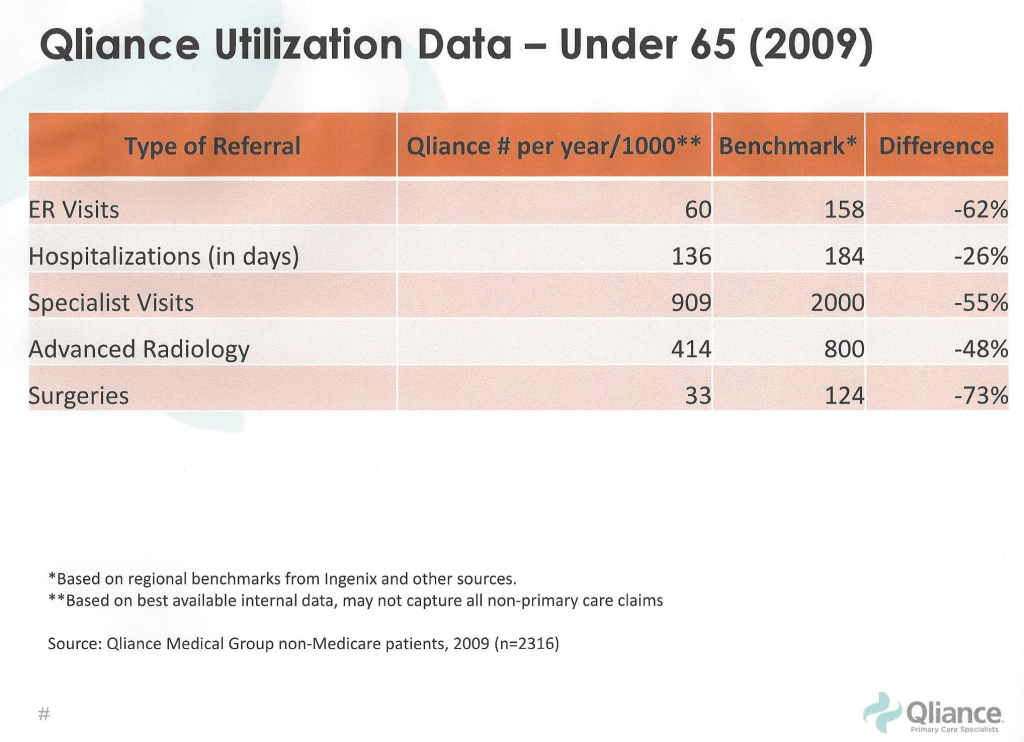
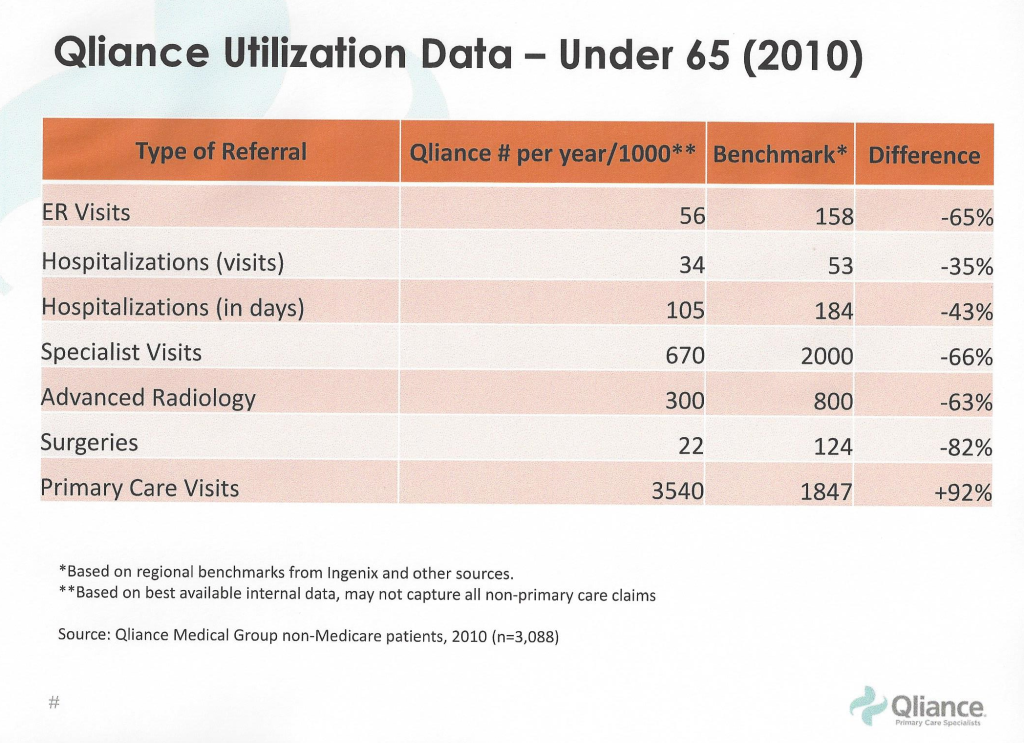
First, one of the main benefits of the direct primary care model is physicians have more time to spend with their patients to actually figure out what is wrong and treat problems appropriately; and therefore, they need to refer patients less often. As family physicians, I believe we are well trained to handle the myriad of problems that patients may present with, but we do not have enough time to adequately address them in a 10 minute office visit, so we often feel compelled to refer them to specialists. QIiance has demonstrated that when you have the time to spend with patient, specialist and ER visits, surgeries and hospitalizations are all significantly reduced
Second, even specialists are willing to reduce their fees when they are guaranteed payments in a more timely manner. Again, when we eliminate the insurance middleman, we significantly reduce the uncertainty and/or time it takes to pay for services. In reality, fees for sub-specialty visits, services, surgeries, etc. are set for insurance companies who routinely underpay by a significant amount, since they can negotiate much lower payments. Again, if we could eliminate the “insurance bureaucracy tax” by reducing administrative costs through the removal of the insurance middle man, specialists could charge patients much less for the actual services they provide.
The original article can be found here from The Direct Primary Care Journal
The Home Visit: Bringing It Back

Yesterday I did a home visit for one of my long time patients that recently got discharged from a Skilled Nursing facility. She has a very complex medical history and has been in and out of hospitals and rehab facilities over the past few years. She is frail and elderly and getting to her dialysis sessions three times a week takes a lot of energy out of her. So why is it necessary for her to expend a lot of energy and experience pain to physically come in for a visit to see me? The answer is it’s not anymore.
See… in the current medical system doctors and nurse practitioners only get reimbursed by 3rd party payers if the patient physically comes in and meets with the doctor face to face. The doctor sees a complex patient like mine for 10-15 minutes if lucky (or if longer end up an hour behind), and then spends a majority of time documenting and coding the visit in order to get paid. Sounds great for the patient and doctor huh? Not exactly. It doesn’t work and it makes no sense.
So that brings me to yesterday. Since I no longer have to see 20-25 patients a day like a machine, I now have control over how I practice medicine and the type of care I provide. By contracting solely with the patient, I can drive 2 minutes to my patient and see her at her home. I spent 70 minutes with her and her children. We reviewed her discharge paperwork, her multiple medications (trying to taper her off a few), and discussed any current issues or concerns they had. I then wrote a brief note documenting the plan and emailed the specialists involved with her care to update them as well. The focus was and is solely on THE PATIENT. All of her and her families questions were answered and we have a solid plan in place to prevent her from ending up back in the hospital- a place she dreads and I don’t blame her. Now we can work as a team to be proactive rather than reactive. We can work towards solid pain management, reduce unnecessary medications and testing, and keep her home where she is safer and more comfortable. Her quality of life is significantly better because her care is better.
And what did I receive in return? A great deal more than $30 or her monthly fee of $125. After 8 years of caring for this woman I got to see her in her ideal setting- her home. I got to learn about the little toy animals she keeps as her hobby. I saw her family in action taking car of her and making her quality of life the best possible. Carpets have been removed so she doesn’t trip with her walker. She has a bell so she can ring in the middle of the night if she is in pain or needs something. And now she has her physician capable of coming to her and spending over an hour with her to make sure she is heard and cared for with dignity. So I got a lot more….I got to be a doctor. Not a bad value proposition for the two core people that make medicine tick- the patient and their doctor.
What We Strive For With DPC

One of the main reasons I decided to make this huge career change into a Direct Primary Care practice was to give patients what they deserve from their doctor….time. One of my patients that followed me from my old practice has allowed me to post this wonderful testimonial she wrote on Facebook on Friday. Many thanks to her for doing so. This is an example of what true patient and doctor satisfaction are about:
“Today I had my first official appointment with Dr. Jeffrey Gold at Gold Direct Care. It was a phenomenal experience. His new office space is beautifully decorated and comfortable. Dr. Gold spent quite awhile with me, answering numerous questions and making me feel, as he always does, at ease. Has anyone ever gone to their primary care doctor and been greeted with: “Would you like some coffee or tea?” My visit was an experience- not rushed, not pressured to hurry up. If you want a primary care doctor who sincerely cares about you and your family and is in the practice of medicine to do just that, then you have to meet with Dr. Gold and see what Direct Primary Care is all about.”
Open Enrollment: What to do next
For all of you who are in the enrollment period for employer-based insurance, including town employees, we can help answer your many questions. We offer free one hour consultations to help look over your insurance benefits. We also show you how Gold Direct Care can complement your insurance in a way which accomplishes two main goals:
1) Provide you with better access to primary care (AKA better quality care) with a doctor that is available to you when you need them. Appointments guaranteed within 24 hours and no insurance hassles.
2) Lower your cost. By combining our aged-based monthly fee with a lower premium/higher deductible plan we can get you to either break even for better value or, best case scenario, we can save you money all the while keeping you protected medically and financially.
We understand how complex insurance options can be. We are here to help you become a better consumer and navigate these complexities, so you and your family are protected; all the while getting the best value for their dollar. Please contact us for any inquires and to set up a time to talk at info@golddirectcare.com or 781-842-3961.
We also have knowledgeable insurance consultants as well whom we can direct you to if needed.
Here is an article with great examples if you would like to learn more: What Really Happens When You Cut The Red Tape
Tufts Family Medicine
So today I spent an hour speaking about Direct Primary Care to 1st and 2nd year medical students at Tufts University that are interested in Family Medicine or Primary Care in general. It was a great experience to see students engaged and interested in pursuing a field of medicine that desperately needs young, bright, and energetic minds. They asked intelligent questions and hopefully learned that there is hope on the horizon for primary care. There is a currently a shortage of good primary care physicians across the country, but especially here in Massachusetts. We need to fix this and the only way to do so is to make Family Medicine palatable, financially rewarding, and most importantly gratifying by focusing on patient care. Read this article from 2013 for more information: http://www.beckershospitalreview.com/hospital-physician-relationships/primary-care-shortage-dire-in-massachusetts.html
Direct Primary Care, in my opinion, is a way to build off the positives of our healthcare system and simultaneously remove the bureaucracy and red tape of insurance that does nothing to help patients or control costs. We have a solid foundation to work off of, but we have to modify it without scrapping the whole construct. DPC does this. It allows insurance to be used the way it was intended to be used- for catastrophic, high cost events or illnesses.
In my hour with them today, I hope I was able to show the students that if we keep fighting the good fight and do the right thing, maybe someday DPC will become the norm rather than the exception. I hope the more than 200 patients we have enrolled already can attest to the value and quality of this old, yet new, model of primary care.
As Albert Einstein once said the definition of insanity is doing the same thing over and over again and expecting a different result.
A Different Kind of Plan
Marblehead’s Gold boosts Direct Primary Care plan – Itemlive.com

MARBLEHEAD — Direct Primary Care is a concept based on the idea that physicians should be dedicated to their patients, and care for them based on their needs, not their insurance plan, says Dr. Jeffrey Gold.
The concept strives on building strong patient/physician relationships and eliminating third parties, such as insurance companies, for primary care.
Many believe it’s a solution to a lot of the problems we see in the primary health care system: waiting time, high costs, and not understanding treatments. Gold is one.
“Let’s get back to using health insurance for what insurance should be used for: the big things, the unexpected things, surgeries,” said Dr. Jeffrey Gold of Gold Direct Care in Marblehead, “not the day-to-day primary care which is expected and what people need.”
Instead, DPC offices charge a fixed monthly rate and provide patients with unlimited doctor visits and unlimited time during each visit. Doctors spend more time with patients and are able to provide a wider variety of care so that most procedures can be performed in the office, Gold says.
When a patient does need to be referred to a specialist, DPC doctors communicate extensively with the specialists in order to ensure the best care for the patient. “When I do refer out, I have a much better dialogue with the specialist,” said Gold.
“I have better referrals, because I’m not referring as many people out and I can communicate with the specialist because I have more time,” he said. “This results in better care for the patient, which is the ultimate goal and should be the ultimate goal.
“This is getting back to what medicine is supposed to be about, which is the patient and physician relationship,” said Gold. “The doctors in the program are trying to provide quality care but the current system doesn’t allow it.”
This method is an attempt to stray away from the traditional medical system, which Gold says has become more about “how many people you can see rather than the quality of the care.”
“Our goal is to help the patient,” he said. “It’s difficult when you’re in a room seeing 20 people a day. That’s not why I went to school for so long.”
Gold aims to have about 750 patients as opposed to the 2,500 he had when working in traditional medicine. The purpose, he said, is “for the patient to really have a lot of questions and be more engaged with their health. I have the opportunity to do that.
“It’s gratifying to spend time with people that you genuinely care about and make sure they are getting what that they need,” he said.
While DCP does not involve insurance directly, a membership does not take the place of insurance. It’s important to know that you still need insurance for emergency situations and surgeries.
“DCP is not insurance, it’s a service.” Gold said.
“All primary care services are included under that fee. I can still take care of someone who doesn’t have insurance but I would never encourage someone to not have insurance. We recommend a high deductible plan so that you’re covered in all aspects of your care.
“We’re trying to work with insurance companies to get the right plan for people. Get them higher quality care,” he said.
While eliminating insurance all together is not recommended, the idea behind DCP is to remove it at the primary care level.
“I work like a gym membership; people can use it or not use it but they’ve paid for the service,” he said.
“Patients pay “a monthly age-based fee that pretty much encompasses 99 percent of what I do in the office,” he said. Falling under the remaining one percent are things like blood work, routine women’s health screenings and even house calls, which Gold says range between $3-$30.
According to Gold, there are many added benefits of being a patient of a DPC office. Doctors have 24/7 availability. They give patients their cell phone number, giving them the option to call, text, email, FaceTime and skype.
“I can talk to a patient on the phone from the comfort of their own bed,” said Gold.
For Gold, it’s about changing the experience patients have with health care.
“Nobody wants to go to the doctor and we’re trying to change that,” he said “It’s up to us to try to fix this and make it better and the only way to do that is to think outside the box and make things simpler.
“It allows for people to have a say in what they’re getting and how they’re getting it,” he said “I hope we get to the place where people demand better and get better.”
