Category: Direct Primary Care
Our Obesity and Healthcare Epidemics: How They Go Hand in Hand

We all should know by now that we have a major obesity epidemic in this country. The best way to reverse this epidemic by controlling our weight and reducing our risk of diabetes, high blood pressure, and vascular disease is by eating real, unprocessed food. Doctors, nutritionists, and other healthcare providers often advise patients to shop the periphery when in a grocery store. Why? Because that is where the real food is. That’s where the produce, the real dairy products, fish, chicken, and meats are. Now, not all of these are truly healthy products which is beyond the scope of this post, but you catch my drift. If you shop the aisles and try to read the nutrition facts you will see my point. For example here is the nutrition info for Cheerios with Protein:
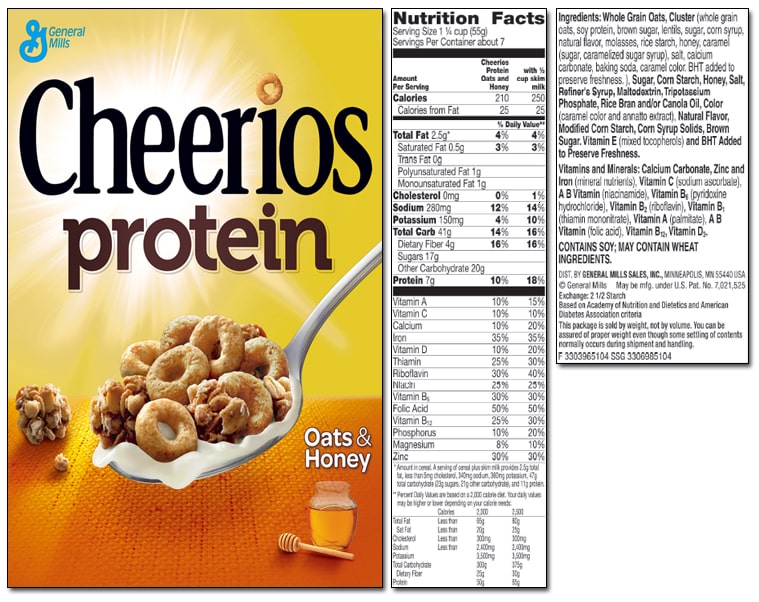
This may seem healthy on the front but look on the back and see that there are 41 grams of total carbohydrates and 17 grams of sugar! Even more interesting to point out is why is sugar one of the few items that does not have a daily percentage value next to it? Hmmmm…..Obscure. And look at the number of ingredients listed- most of which can not even be pronounced. All in all….not good and certainly not healthy. Real food is always the better option.
It is also recommended to try to cook and eat as home a much as possible to help you get or stay healthy. I am by no means a master chef but based on my experience whenever I have tried to make some complex recipe with a lengthy list of ingredients it has turned into a complete inedible mess. Ask my wife about the spice-rubbed pork tenderloin from Epicurious I tried to make a few years back…god awful. Yet, every time we use a recipe from Cooking Light it comes out great. There are fewer ingredients and fewer steps for one to screw up. It is simple, healthy and usually quite delicious. I’ll leave the complex recipes and dishes to the master chefs.
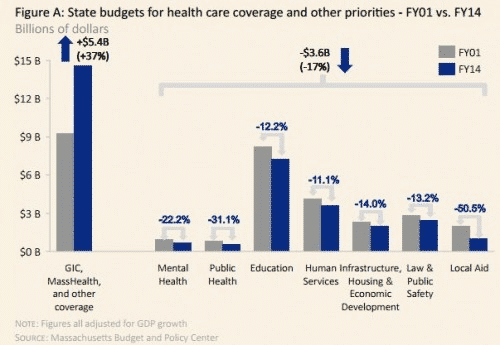
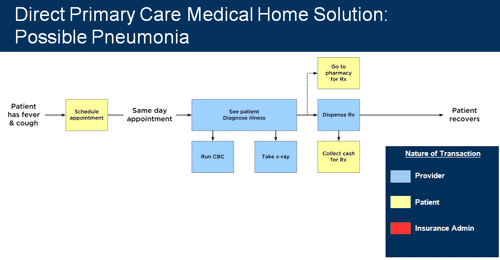
Hopefully by now you can see how this is going to tie in to our Healthcare Epidemic. Our system has become so bloated and complex with way too many needless ingredients and cooks in the kitchen that we can’t get out of our own way. See the proof here as our own state of MA spends 40% of the budget on Healthcare at the expense of other important needs:
While we keep adding layers of red tape and bureaucracy, as well as continuing to allow third parties (government and insurers) to set quality measures, create networks (i.e. doctors and hospitals whom you can and can’t use), and set nontransparent prices, the doctor/patient relationship- you know… where the actual care and medicine takes place- will continue to suffer. You will have less access, longer wait times, less time with your doctor, and more visits to an Urgent Care clinic. Is that really what people want for their healthcare?
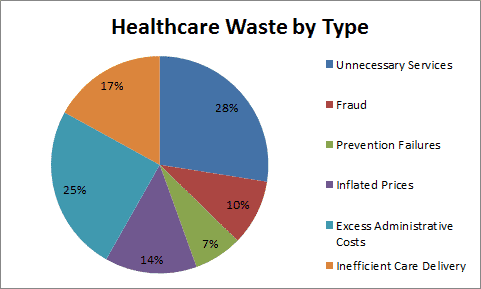
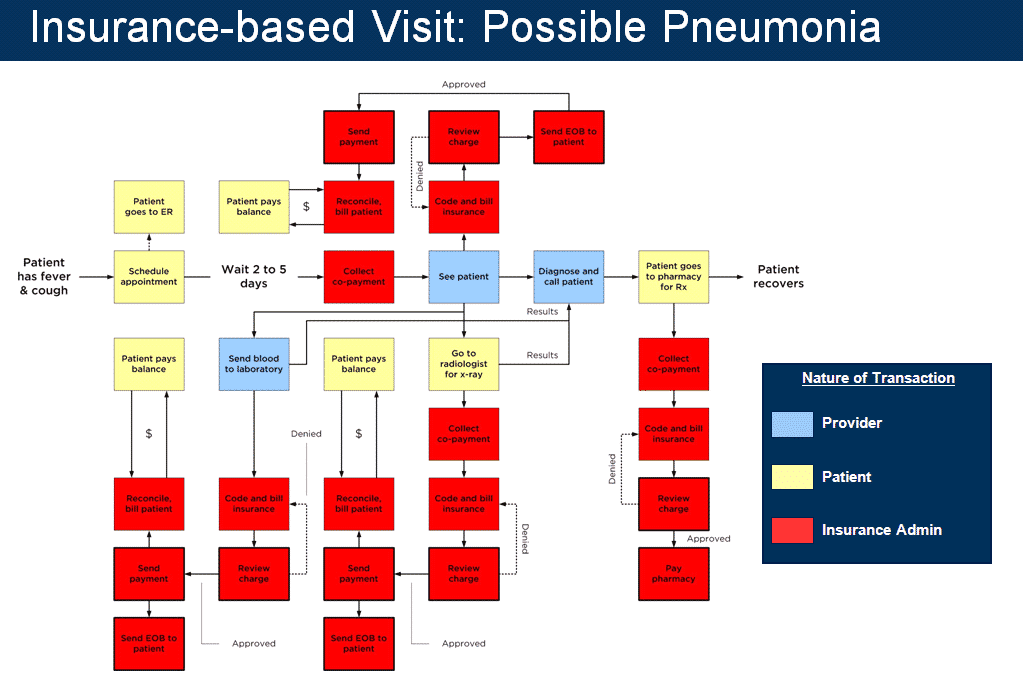
In conclusion, healthcare- especially primary care- does not have to be so expensive and complex if we just get rid of the wasteful ingredients. Let the patient, the actual consumer of the service/care, determine value and not a third party whose goal is profit and profit only. Let insurers be true insurers. Let government provide financial aid to those whom truly need it, but stop practicing medicine. Let the doctors practice medicine without layers of regulation and trust me, the bad ones will show themselves. In healthcare, just like with nutrition, the saying “less is more” could not be more appropriate. Just look at these these diagrams to see how DPC changes the recipe. *mic drop*
Why Are We Paying So Much Money For Health Insurance When We Still Can’t Afford Care?

The Boston Globe published an article on March 23, 2016 titled Even With Insurance, Mass Residents Often Can’t Afford Healthcare and I can’t even begin to explain how true this is. They really hit the nail on the head with this topic! Being a young adult, I can completely relate to what it’s like to not be able to afford health insurance. Not until last year did I really begin to understand how expensive health insurance really is. I started working for a big company which offered “the best” health insurance (no need to mention names). I was so excited to think I had this ‘top of the line’ health insurance. It was all great until of course, I made my first visit to the ER. With a very expensive co-pay, high deductible, and multiple bills later, I realized how unaffordable healthcare truly is. Just as this article states, having health insurance doesn’t necessarily mean you can afford care. I immediately noticed- yes, I finally have “great” health insurance, but does it even matter when I can’t afford to go to the doctor? With the statistics from the survey BCBS conducted, clearly I’m not the only one in the same boat. As mentioned in the article “43% of people said in 2015 health care and costs had caused problems for them and their families, including 19% who went without needed care as a result.” How crazy is it that almost 50% of the people surveyed have issues with health care costs?! That’s a huge percentage, which includes me, and possibly you too. We already have so many bills to pay and stress about, healthcare really shouldn’t be one of them. Another thing I noticed from the article are the comments being posted. So many people are complaining about this issue, yet they don’t want to do a single thing about it or, perhaps, they don’t know of other options out there. I think it’s time we start doing our research as healthcare consumers and see what other options we have out there!
This article really struck a chord with me, especially now knowing about Direct Primary Care and really understanding what it is. I wish I would have known about DPC earlier, or even know DPC was an option. Of course we do still need health insurance, but why not choose DPC for our primary care needs? This way we don’t have to deal with co-pays or high deductibles from our health insurance, not to mention getting more personalized care, appointments in a reasonable amount of time and honestly, a real connection with your doctor. Why wouldn’t you want a real connection with your doctor?! They are the ones who are dealing with a big part of your life; your health. The article from the Boston Globe should really relate to many of us, and also be an eye opener. With the results from the survey by BCBS, we can’t deny health insurance is way too expensive and we just aren’t receiving the best care for the amount we are paying. Instead, we end up with a huge headache because of very high bills and often poor to mediocre healthcare.
Written by Jessica Leon, Administrative Assistant; Gold Direct Care
Direct Primary Care: A Medical Students Perspective

As the end of our first year of medical school approached, we received our assignment for where we would complete our primary care apprenticeship for the following year. After the countless hours of studying in isolation, we would finally be fully emerged in a setting to interact with patients and be able to put a face to the multitude of diseases and medications that we spent learning in the prior months. Before our first day at Gold Direct Care, we only had our own experiences as patients as well as the opinions- both positive and negative- from doctors and upperclassman to guide our perceptions of what it would be like to be a primary care physician. Among opinions of fellow classmates, rarely would we hear, “I want to be a primary care doctor.” As for physicians, a compilation of their opinions illustrated the picture of the primary care physician as a half assembly line worker and half paper pusher. Furthermore, in order to provide the best possible “patient centered care,” there were certain rules set by administrators and insurers. Everyday you will see 26 patients. For each appointment, you have 15 minutes to obtain an accurate and complete history and physical exam, strengthen the doctor-patient relationship by establishing rapport and find the time to teach medical students and residents. And the reward for successfully juggling all of these tasks is a stack of endless paperwork waiting to be completed.
As we walked through the doors on our first day, the dreaded barriers that we envisioned were nowhere to be found. In fact, we quickly learned that Direct Primary Care (DPC) and Dr. Gold operated by a different set of rules. There was no time limit for each appointment and the length was determined by no one other than the patient. Thus, there was not only more than sufficient time to address all of the patient’s wants and needs, but also to establish a strong rapport in order to strengthen the relationship between the two most important people in healthcare, the doctor and the patient. Since Dr. Gold never had to worry about a stack of paperwork, he was able to reallocate that time towards teaching. Specifically, we had the opportunity to interview every patient, perform a detailed physical exam and properly document the encounter while being supervised and guided by Dr. Gold in order to maximize every learning opportunity. While these may just seem to be unique characteristics of Dr. Gold, it is the environment created by DPC that allows great people like Dr. Gold to be great doctors to their patients, as well as great teachers to their students. After our experiences working at Gold Direct Care, the negative picture of primary care that we originally envisioned had transformed into one that any current or future doctor would desire.
With a desperate need to attract more medical students into primary care, students are still reluctant to pursue careers in primary care. Dr. Gold and DPC offer solutions to this problem. Doctors can practice medicine the way it ought to be practiced, which is solely focused on the doctor and the patient. Instead of working for an insurance agency, you get to work for your patients, who will ultimately determine your value. No more paper pushing, no more assembly line, just the doctor and the patient working together to improve health outcomes- a recipe that will make primary care a very attractable career path for medical students once again. After arranging an information session for Dr. Gold to share the benefits of DPC with our class, it was quite evident that we were not alone with our enthusiasm regarding DPC. In fact, shortly after its conclusion, a fellow student sent us a text “Guys, I think I want to do primary care now!”
Thank you to Dr. Gold and Meghann for this incredible learning experience. Everything you taught has been invaluable and will help shape our future careers in medicine. Also we would like to thank all of Dr. Gold’s patients for allowing us to learn through hands on experience and giving us advice that will help improve our abilities as future physicians.
Michael Held & Douglas Rodgers
Tufts Medical School Class of 2018
A Win For Gold Direct Care and DPC in MA

![]()
Direct Primary Care is written into the Affordable Care Act as an approved method of receiving primary care as long as it is combined with a catastrophic insurance plan. (Isn’t that how insurance is supposed to work? But I digress.) The ACA clearly defines that DPC is not “insurance” and purchasing a DPC membership alone does not meet the standards of being “insured.” It is required to purchase at least a high deductible insurance plan along with it to be qualified under the ACA. See great article on this here: DPC Clause in the Affordable Care Act
However, on the State level, many legislators, policy makers, and Department of Insurance commissioners want to claim that DPC is the “business of insurance” and should have to pay licensing and regulatory fees. In other words, paying a reasonable monthly fee for all your primary care needs should be regulated no different than Blue Cross Blue Shield, Harvard Pilgrim, etc etc. Having to pay fees of this magnitude would clearly put a small DPC practice like us out of business. We are not “insurance”. We are a primary care medical practice that chooses to work solely for our patients- not third parties- and therefore be compensated by our patients for what we believe is a reasonable monthly fee. About 15 states in the US have now passed legislation stating this as law. Massachusetts is not one of them and has yet to introduce a bill that by stating such protects us and our patients who choose us. We, along with three new DPC practices in MA, are tirelessly working on getting our legislators to listen to us and sponsor a bill.
As the first DPC practice in MA we were contacted by the Massachusetts Department of Insurance when we first opened in January 2015. With our legal counsel we have met with them and corresponded with them on this issue. It has been months of waiting and practicing medicine in an unclear regulatory environment. This weekend, much to my delight, I was contacted by my attorney with a letter from the DOI that has given us the green light to continue practicing medicine without 3rd party interference. (The letter is attached below a sit is a public document.) We are very thankful to Commissioner Daniel Judson and Deputy Commissioner Kevin Beagan for their understanding that what we are trying to do is solely for the benefit of the people of Massachusetts and the primary care doctors who want to care for them in a manner that echoes the “olden days of medicine.” Hopefully there are better days ahead for healthcare in Massachusetts. (more…)
It Was the Best of Days and the Worst of Days

Last Wednesday, January 6 2016, was a day I will not forget any time soon. It was a day that showed me the worst of our healthcare system but also the best. The week prior, a new patient enrolled with us online. His name was not one that was familiar to me. We scheduled him for a full checkup the next week. Patient X is a 29 year old male chef that found me online because he had no health insurance and was looking for an affordable entryway into our healthcare system. He had applied for Medicaid but was waiting on confirmation. He is a hard working, honest guy that could not afford to purchase any of the “affordable Obamacare plans” on the exchange. Luckily, he did qualify for subsidies to get MassHealth but he was not confirmed at the time of our visit. For this, I will thank Obamacare. It is not bad in every way.
After my nurse put him in the exam room and got some information on him she came back to my office to tell me about the multitude of symptoms he had been having for the past 4-6 months. These symptoms had worsened over the past few weeks and finally prevented him from working. These symptoms included left sided headache with blurred vision in his left eye, bilateral hip pain, back pain, some weight loss, and an enlarging lump in his testicle which he attributed to an enlarging benign cyst that was diagnosed by another physician years prior. Clearly he was anxious and you know what? So was I.
As I entered the exam room I was greeted by a tall, slender and very personable young guy. We walked through the details of his symptoms and the time course. I encouraged him to relax and take his time since with Direct Care there is happily no more rushing through the mill. Needless to say his story was very concerning to me and it was amazing to me that this guy was able to perform labor up until two weeks prior, especially since the pain was keeping him up at night. After his history, I conducted a thorough head to toe exam. He only had minimal neurologic findings. When he was lying down so I could examine his abdomen I could see a large left sided mass in his groin under his shorts. Sadly, all the worst-case scenarios that were running through my head were now close to being confirmed. As he stood up and lowered his shorts I was presented with the culprit- a large left sided testicular mass with swollen nodes in his groin- i.e. it had already spread and now I was concerned that all his other symptoms were manifestations of the same. This was not an easy conversation to have but I sat with him and relayed my concerns.
So the first worst part of the day was seeing this guy suffer with awful symptoms for so long without engaging our system. Was it fear of illness that kept him away? Fear of cost? Denial? Truthfully it was probably a combination of all of the above. The hard part for me was seeing the regret on his face. I tried to reassure him that what is done is done and we can not go back in time, but that we need to deal with the here and now and move forward. And so we did.
So now for the best part of the day. Within 20 minutes our wonderful insurance broker, George Claassen, came over to the office to meet with Patient X and get his insurance confirmed, as I knew he would be heading for extensive and expensive treatment- the stuff for which insurance should be used. While he met with George, I was on the phone with a great local urologist who agreed to see the patient that afternoon and was willing to do a cash price for him if needed. Following his visit the patient called me and told me it was advised that he would need CAT scans the next day prior to urgent surgery that was scheduled for Friday AM. Thank god we got him on insurance right?
That is until he told me that his new Medicaid plan would not cover the CAT scans- CAT scans ordered by a specialist with years of experience that is CONTRACTED with MassHealth!- the second worst part of the day. He was told by the schedulers at the hospital that the order needed to come from a MassHealth PCP! What planet am I on? A specialist nor an MD who diagnosed his condition can’t order an outpatient scan because of what?… Bureaucracy of course. I will not bore you with more details as the situation ended up working out and he got his scans the next day- which sadly showed spread of disease to bone, brain, nodes etc- and he had surgery last Friday. He is now in the hospital with a long arduous road ahead while he awaits chemotherapy. His pain is under better control and all we can do now is hope that his strong constitution and will to get better will guide him to being fully cured. But did he really need the two hours of aggravation after being told he had bad disease?
So like I said…it was the best of days and the worst of days all wrapped into one. It glaringly showed the positives and negatives of our system in the USA. All I hope for is the “best of days” when I can say that Direct Primary Care- for 50$ a month- saved the life of a really nice, polite, hardworking, appreciative, 29 year old year guy. It is an honor to be his doctor.
Disclaimer: this was written with the patients consent and he approved its content prior to posting.
Opiates: A Painful Topic For Everyone

Todays Boston Globe has an article regarding physician prescribing of opiates to patients that have already experienced an overdose Opiate Prescribing to Patients With OD History. Between the documentary that HBO aired last night regarding the opiate crisis on Cape Cod and this article from today, I felt that as a primary care physician and as a resident of a seemingly “white-picket fence” suburb of Boston that has experienced its own opiate epidemic with the loss of too many good people- many of them kids-to this illness, it was worth commenting on. Many of these kids and young adults I knew and even played street hockey with as a kid. Others I did not know at all, but I can feel the loss when something like this happens.
I am not an Addiction Specialist or a Psychiatrist but as a Family Physician we do often deal with these issues and are usually the front door to the healthcare system. I have treated many patients that struggle with the disease of addiction and it is an extremely complex disease that is extremely difficult to cure and it usually coexists with other mental health diagnoses whether it be ADHD, major depression, anxiety disorders, bipolar disorder etc etc that add to the challenge. The hardest part of the disease to address initially is the denial. As a key cog in the wheels of this disease, denial is the toughest nut to crack. Just like any other chronic disease we treat, patients have to come to some degree of acceptance to move forward, and with addiction denial prevents this from happening easily. Sadly, we have no idea when that bridge of denial will be crossed and what the outlook on the other side looks like, but it needs to be crossed nonetheless.
I may be an idealist at heart and obviously have my biases, but I think one key solution to this epidemic is better primary care. People that struggle with the disease of addiction obviously need a multidisciplinary approach- one that includes doctors, nurses, social workers, counselors, addiction specialists etc- but they also need a primary care doctor that can help them navigate this messed up system, be the teams quarterback, and most importantly know them and treat them as a human being rather than just a “disease”. We need to ask the hard questions such as “with all the stories and news out there on this issue, what drove you to take that pill that started it all? what support system if any do you have? how can WE help YOU get healed? How do we as a community band together to educate and support our kids in a nonjudgmental supportive way? What are WE as a community doing wrong?” It isn’t all about the actual drug or the patient and the choices they have made. Its an US issue because it could be any of our friends, family members, or children that can succumb to this disease. And I don’t know about you but aren’t you tired of reading these obituaries week after week?
Our primary care system and mental health system need an overhaul for many reasons, but this epidemic is a big one. All patients of all socioeconomic backgrounds that struggle with this awful illness deserve better than 15 minute visits. They deserve better than more pills thrown at them. They deserve a relationship that is based on trust, care, and respect. What if the doctors that were studied in the aforementioned article had time to research records and databases during these visits? What if they actually had time to call other members of the patients care team? What if they had time to discuss the risks, benefits, and alternative options for pain management with their patients with appropriate, close followup and communication? I can personally attest to the fact working in the Direct Primary Care model has allowed me to treat patients with addiction 100% better. I have the time to listen, call other resources if needed, and followup frequently by phone or email. I am by no means perfect and do not always have success sadly. Yet there is one thing that DPC has allowed me to show the patient who struggles with addiction that all the Continuing Medical Education and seminars in the world do not even touch on and that is……that I too am an imperfect human being, that I do care, and that there is hope. I know this idealistic view will not solve the whole crisis, but maybe infusing some humanity towards these patients is a good start towards helping them heal and live a healthy life? What we are doing certainly is not enough and to me that is unacceptable.
Happy Thanksgiving- A Honest and Heartfelt Thank You Note

It amazes me to think that at this time last year, though Gold Direct Care was so close to becoming a reality, it was still in many ways a figment of my imagination. So it is in a state of disbelief and gratitude that I’m writing this post, focusing on what I am thankful for this holiday.
I chose to leave the “established healthcare system” after 10 years of practicing in it, because I knew there had to be a better way to give and receive care. The two key groups of people who actually make the healthcare system breathe- the doctors and the patients- deserved so much more and so much better. I realized the only way I could possibly make a positive change and deliver care in a better way was to leave the existing, broken system and hope that others would follow. I hoped the level of care and the relationships I had nurtured with my patients would trump the admittedly steep curve of subscribing to a new model. As I well know, change can be hard even when it is a positive one. Despite huge opportunities for cost savings ( read post by Dr Patrick Rohal from Lancaster PA here: Why In the World Would I Pay TWICE for Healthcare), I worried it might be difficult for my patients to feel comfortable paying out-of-pocket for some services. Then again, I also figured so many people would be thrilled to regain control of their health care and health care dollars that they would jump at the chance to improve on our existing, personal doctor-patient relationship. People seemed to crave “old-school” medicine. I heard all around me patients talking about the value of “good” health care – this made sense.
It was never out of egotism, rather out of the work and care that I had given to my patients that made me believe a significant number would follow me. I had 2,500 patients or so on my “panel” and knew that I would need around 700-800 to make a Direct Primary Care practice sustainable. So, in the first couple of months, when only a hundred or so patients moved to the new practice with me, I wondered if I had been wrong. Had I deluded myself into thinking I was more valued by my patients than I actually was? Did people truly want a better relationship and more access to me as their physician, or is that just trendy to say? Were people honest when they talked about how important excellent care was to them? Had I misread everything?
I had invested so much into my patients and tried my best to develop real relationships with them, albeit in rushed 15-to-20 minute “traditional healthcare model” intervals, that I believed the same was felt on their part. See, what I always valued most was not my salary, but the privilege to take care of people. Yes, I like money just as much as the next person but let me tell you, med students do not choose a career in Primary Care for money. They choose it for the relationships with people. That’s why I chose Primary Care. I wanted to develop real, longitudinal relationships with my patients and truly care for them…providing that real value that they were saying they wanted and that everyone deserves.
But at the end of the day, value is determined by how much we are willing to spend on something. And so from January through about April of this year, I felt quite devalued as many of my patients elected not to pay out of pocket to keep me as their doctor. I share this, not to make anyone feel bad for making that choice. People have a variety of reasons for the choices they make- especially in a scary and complex industry such as Healthcare- but it was quite hard not to take this choice personally. I mean, medicine, particularly primary care, is personal after all. So please understand that I share this solely as an honest description about what I felt and how I viewed things at the time. I have looked at this from all perspectives as I too am a patient after all.
When pricing for my services, I tried to be as reasonable as possible without selling myself too short. I wanted to be accessible to my patients while developing a sustainable business model that supports state-of-the-art facilities and equipment, an unbelievably convenient location and – most importantly – time. If I was to be the change in the broken system, I needed to make sure the new model was set up to allow me and a growing team the time to nurture patient relationships and provide real primary care. The end result was that I settled on a maximum of 125/month, which is less than most monthly cable bills and a coffee a day if you look at it from a dollar perspective. Surely people who had been crying out for better care, better access, better Doctor relationships, less wait times, less frustration, less – well – crap would consider this a huge value. So to put it bluntly and honestly, I often felt heartbroken during those months.
After those few months of feeling sorry for myself, focusing my energy on why I now had a huge population of “former patients”, and continuously asking myself , “did I make the right choice here?” I realized it was time to move on. It was time to focus on my mission of promoting the Direct Care model, and working to introduce my practice to new patients. Even more importantly, it was time to spend all of my energy on the 100 or so people that chose to come with me. They deserved what I promised them; it was this core group of people that would determine the success of my practice.
There was never one specific moment or incident that occurred to help me turn that corner and refocus. It was a gradual process of becoming a business owner for the first time in my life and really just growing up. I focused on the positives of the change- such as new patients excited to come on board, seeing more of my old patients trickling back to me, and enjoying my ability to actually doctor in the manner I always wanted.
So here I sit, writing a long thank you note on Thanksgiving Eve to those 100 or so patients that stuck with me right from the start. I hope you read this so you can truly know and understand how thankful I am for you seeing the value in keeping me as your doctor and in my lofty endeavor of fixing a truly archaic and dysfunctional system. It is because of early adopters like you that my practice is growing and thriving. It is due to your willingness to go against the grain that we now have Dr. Mancini with us. It is certain people who dropped a Medicare HMO plan to switch to regular Medicare so that they could keep me as their doctor that helped heal a broken heart and revive my belief in the value I provide as a Primary Care physician. I am so thankful to you and the rest of the Gold Direct Care patients for believing in me and for taking the first step towards a better quality, more humanistic, and ultimately a more affordable healthcare system.
Thank You. Thank You. Thank You.
And finally…a big thank you to my nurse Meghann Dunn who was there from the beginning because she believed in my mission. Our patients and I are very lucky to have her.
Now feel free to go stuff your face with turkey and loads of carbs. Happy Thanksgiving to you and your families!
Dr. Carmela Mancini Joins Gold Direct Care
Hello, I am Dr. Carmela Mancini and I have recently joined Gold Direct Care. I am so excited to be a part of the Direct Primary Care movement! Like many physicians in today’s healthcare environment, I realized that my idea of being a doctor was not possible in the current system. I wasn’t able to spend the necessary, quality time with patients; decisions were often based on what insurance dictated and not what I thought was medically appropriate; there was disintegration of the doctor-patient relationship. This is when I discovered Direct Primary Care and I have not looked back.
I am board certified in Internal Medicine and have spent the last several years as a hospitalist. Prior to medical school I received a Masters degree in Public Health and spent 5 years as a public health advocate and epidemiologist. I subsequently went to medical school at Nova Southeastern University and eared a degree in Osteopathic Medicine. I completed my residency in Internal Medicine at Baystate Medical Center in Springfield, MA.
I am very excited to be accepting new patients. Please contact the office at 781-842-3961 or email me at drmancini@golddirectcare.com to schedule a free consultation.
For those of you interested in learning more about Direct Primary Care please attend one of our information sessions at the Salem Waterfront Hotel (225 Derby Street Salem, MA 01970) on November 9 (1-3 or 7-9) or November 17 (1-3 or 7-9). Go to http://findnsave.wickedlocal.com/Local-Ads/a-634135/Gold-Direct-Care for complete details or call 781-780-2461 to RSVP.
End of Life Care: We Can Do So Much Better (Dedicated to Wilbur)
Ever since I watched my grandfather and grandmother suffer from devastating diseases like diabetes and dementia, I have always been passionate about how we treat people at the end of their lives. With all of the technology, specialized medicine, and wonderful hospitals we have in this country we often never know when it’s time to stop using them. As physicians, we are so afraid of losing patients (i.e. failing), and death and dying in general, that we often lose sight of “life and living”. Sometimes the best medicine is to not only let people go, but more importantly to let them go on their own terms.
Yesterday, I lost of one my longtime patients and supporters- Mr. Wilbur Basset at the age of 89. (I am using his name and picture with permission from his family.) Wilbur and I met when I first moved to practice in Marblehead 8 years ago. What struck me about him was both how healthy he was for an older man, and even better how incredibly sarcastic and funny he was. I always enjoyed that he was for lack of better terms “a curmudgeon”. He never complained unless something was truly bothering him. It took 8 years, and me removing myself from the factory mill of modern day healthcare in order to move to the Direct Care model, for me to actually meet his family and spend time with them. I am so glad that they stuck with me and gave me the chance to show them what medicine can be like.
Unfortunately, over the past few months Wilburs illness and condition worsened. I saw him in the office with his daughter a few weeks ago and I could tell that he was declining. Given how stubborn he was, he always fought through stuff, but this time he just looked different. As I helped him in the car he said “I am so ‘blanking’ done with this.” I just knew he was ready. So after his daughter and I had a great chat about consulting with Hospice, he sadly ended up in the hospital before we could get the consultation scheduled. When I visited him there I could see how miserable he was. After a week or so, which of course included a few unnecessary consults, he rapidly worsened and was transferred to the Kaplan House where he peacefully passed away with family by his side after a day. Fortunately I got to say my goodbye to him yesterday.
As a system, we have to do better for patients like Wilbur and their families. We must do better. For me, I will always remember him the way he was a few weeks ago, and I will always be thankful to have had the opportunity to care for him and his family through his journey. I may not be a specialized surgeon or a cancer specialist, but I am so thankful that Wilbur and his family went Direct Care with me and granted me the most gratifying job in the world. I was his doctor.
Rest in peace Mr Bassett. You have earned it and did it on your terms.
ICD-10: It’s Nice Not Knowing You
Today, October 1st 2015, is a very critical day for the “disease management” system that we mistake for a healthcare system in the United States. Today is when the new coding system called ICD-10 goes live for a majority of American physicians and Nurse Practitioners. This is nothing more than another layer of bureaucratic red-tape that does nothing to enhance the quality or cost of your care, but rather furthers the disease process. All it does is waste more of your physicians and office staffs time- time that should be spent working towards your care. Instead it just feeds an already broken machine that is aimlessly running on fumes while blowing exhaust into the faces of the people whom matter most- the doctors and the patients.
Luckily for us and other brave practices and patients across the nation, we have nothing to do with this nonsense. We have decided to escape the mess and fix medicine from the ground up. Our focus is solely on working together towards a system that actually makes sense and works for our patients. This is what gratifies us most- being able to provide care the way we trained to do. So help us raise awareness about the Direct Primary Care model today- National Direct Primary Care Day! Check out the following link, share it, talk about it, and maybe even buy a t-shirt:
And finally, here’s to being part of the solution rather than adding to the problem. We thank you for your support and for being willing to do one of the hardest things for anyone- change.

