Author: admin
Save the Foundation of Healthcare…..Please Shop Local and Help Pave a New Path

Image credit to Frostburg MD
I am not writing about Covid-19 to make it a political issue (it’s not), to discuss what we should have and could have done better (hindsight is 20-20), nor am I writing about it to discuss all the fatalities and lives that have been adversely affected by it. It has been devastating for many people of all walks of life in so many ways- death, isolation, loss of income/jobs, loss of savings, etc etc. All these facts are known. The reason I am writing on Covid-19 is to try to see the hope in the devastation that it has caused. We as a society have a chance to better for ourselves and our children. We have seen the best and the worst of our society during the past few months. My hope is that we can be better to each other and for each other- learn how to meet in the middle on all issues, treat each other with respect, and have dialogue that may never end in an agreement, but that ends in mutually respectful disagreement with all parties learning something from one another. One of my favorite quotes is from Ayn Rand, who is admittedly a polarizing writer and thinker herself, but nails it with this one. “When I disagree with a rational man, I let reality be our final arbiter; if I am right, he will learn; if I am wrong, I will; one of us will win, but both will profit.”
With that being said, one thing I hope we can all agree on is that this pandemic has exposed the best of our healthcare system- the doctors, nurses, therapists, CNA’s, janitors, cafeteria workers, maintenance workers, etc that have kept hospitals/ERs operating like well-oiled machines so that people could be treated to the best of their ability, even while putting themselves and their families at risk by working every day with a lack of adequate PPE and support. Many have actually died themselves which I am pretty sure is not part of the Hippocratic Oath, yet they went to work because medicine is a calling not a job. Another aspect I hope we can all agree on is that the pandemic also exposed every aspect of our healthcare system that sucks. We are fragmented, the clinical staff of all ilks are underpaid and undervalued, we are overly expensive, and we are always reactive to everything rather than proactive. Ultimately, we don’t have a healthcare system, but rather sadly a “sick care” system. Being proactive, working to prevent chronic disease, and staying healthy are sadly not profitable nor “sexy”. Filling hospital beds, MRI machines, specialists offices, prescribing expensive drugs, and DOING more TO people rather than less are. Yet there is hope. We have an opportunity to rebuild a healthcare system that our children and grandchildren and generations following them deserve. We need this, but the question is do we want it badly enough? Do we really really want it? If you think we do then keep reading and ask yourself this- if given 5-10 million dollars to build a brand-spanking new ocean side mansion would you put it on top of a leaky, cracking, termite-ridden foundation?
My guess is that your response is a big fat NO. So now ask yourself why in gods name are we doing that in healthcare? Why have we devalued primary care to 7 cents of the dollar and a minute fraction of the spend from public payers like Medicaid and Medicare, from private insurers like BCBS etc, right down to the public itself that believes real primary care can be done well at a drive through clinic? In a ten minute visit? Costs nothing more than a 20-30 dollar copay? Can be done well by any Tom, Dick, Jane, or Harry with a white coat and initials after their name?! And these beliefs are mostly not the fault of you, the general public, as you have been brainwashed and trained over decades by the rulemakers- pharma, insurance lobby and bureaucrats- to believe them. If you do not believe this fact here is a reference: https://www.benefitspro.com/2019/07/26/u-s-spending-less-than-other-countries-on-primary-care/?slreturn=20200428161727 No wonder why our system is not affordable, easily accessible, and navigable?! Yet we- patients and doctors- can fix it. Let me restate that…it is UP TO US TO FIX IT!!!. From the bottom up, we can rebuild a system that works for us. We can be the rule makers. This is our chance for once and for all to stop relying on the wrong rule makers to fix it. As a dear friend and benefits advisor says “you can never win a game where the opposing coach and the referee are the same person. This is how we do it….
This article below was published in STAT news today and discussed how “Covid-19 has devastated independent primary care practices.” Well guess what? It isn’t Covid-19 that devastated it. It is the screwed up, inefficient, overly expensive way that we- or in most cases the way third parties like government, insurers, and self insured companies pay for it- and those dollars all come indirectly from working peoples pockets at hugely jacked up rates! It is what triggered me to write this post and urge people to help us rise like a phoenix from the ashes of this unfortunate nightmare that Covid -19 did nothing except shine a light on. https://www.statnews.com/2020/05/28/covid-19-battering-independent-physician-practices/?fbclid=IwAR17jbNkb02eHKZ0NKHh1Ue_3UiETM9PBsgfB87vSnE853nloCODjmKgk-k
So it is time we s&*t or get off the pot. For five years myself and many other primary care doctors across the country have felt like we are moving a whole beach by ourselves. We need help. We need the public to grab a pail and start moving some sand along with us, because it’s the wet, dirty heavy sand of the Northeast, and not the light, fluffy white sand of the Caribbean. NEWS FLASH! No one else is going to do it for you and if we continue to try to do it on our own we will burn out and fade away (which is already happening at alarming rates). Sorry but thats the reality. A contractor friend of mine says that a foundation of an average home is about 15-20% of the spend. Imagine if we did that for primary care in the US? Imagine insurance premiums that do not cost a mortgage? Imagine transparent, affordable care delivered to you the way you want with a doctor of your choice? All for less than 3-4 dollars a day? One can only dream. We all want change, but we often resist the path to change. Why? Because its freaking hard! So here is my call to action: grab your pail(s), walk with your feet, speak with your words and your wallets (and if you truly can not afford an average of 70 dollars a month for unlimited primary care, discount labs, imaging, meds telehealth visits- yeah hey policymakers/insurers us DPC docs have been doing them all included for 5-10 years so welcome to the 21st century- call your elected officials and demand a health savings account funded with money based on need to use toward primary care with Medicare and medicaid to cover all that happens outside of it). Stop using insurance like a credit card for stuff that doesn’t cost as much as a sandwich. It makes no sense. Join a DPC practice, or at a minimum, use an independent primary care practice that is not owned by an unchained Goliath- aka major hospital system. If you do not like the beast and hate what it has done to you and your income, be a David. Help us starve it until it dies. Find something positive out of the Covid-19 pandemic and act on it. Do it for those we have lost and for our children and grandchildren who did nothing to inherit the ashes of the Goliath that now rest upon the beach we all want. Or please….DO NOT complain. Take the PATH less traveled: https://dpcalliance.org/dpc-path. You may enjoy the hike. If not, I’m sure the cartel of “rule makers” will be there waiting to pull you right back in. “Where’s the tylenol?”
Coronavirus 19 Info and Guidelines
Thank you to Dr. Allison Edwards from KC DPC for her work on a majority of this information.

Good Afternoon,
We are reaching out because we know this is a confusing and anxiety provoking time for many people. As you are likely aware, Massachusetts residents have tested positive for COVID-19 (the illness caused by the novel Coronavirus) and we expect more cases to be identified as testing availability expands over the coming days to weeks. As of earlier today there are a total of 95 presumptive and confirmed cases of coronavirus in the state. Most of the these patients will do very well and will not require hospital level of care.
As your physicians, we are committed to staying up to date on developments and changes, so that we can provide you with the most accurate and timely information possible. We are routinely reviewing updates from the Massachusetts Department of Public Health (https://www.mass.gov/orgs/department-of-public-health) and the CDC (www.CDC.gov). If you have questions or concerns, we strongly urge you to visit and utilize these resources. We do not recommend you get your information from social media.
This is not a time to panic, but we do all need to institute some changes in our day to day lives to try to slow the spread of the virus. Yes, it may be inconvenient, but it is necessary. We may not be able to prevent a large portion of the population from getting this infection, and the majority of people who are infected will do just fine. However, it is very important that we slow the spread so that huge numbers of people are not infected at the same time, which would overwhelm our hospitals’ ability to care for the segment of people who need hospital level care due to severe illness. We ask that everyone practice “social-distancing” and avoid non-essential large gatherings or unnecessary travel, wash your hands frequently, avoid touching your face and stay home if you have a fever or cough. This is the best way for us to ensure that there will be adequate health care resources for folks who do get very ill from the virus.
At Gold Direct Care we are fully committed to caring for our patients in the most evidence-based, safest capacity possible. We want to make sure that you know how we plan to serve you as COVID-19 spreads through our community, so we’ve put together the following information to explain what you can expect from us over the next few weeks to months.
As of today, March 12, we are asking those with respiratory symptoms (cough, shortness of breath, wheezing) and/or fever to first call the office (781-842-3961) or text message your physician. DO NOT walk-in to the office without first calling. If you walk-in you are potentially putting our staff and other patients at risk unnecessarily. We will reach out to you for more information and determine the best way and place to evaluate you. If you have a regularly scheduled visit for a routine, non-urgent issue and you want to cancel in light of current events, please call the office and Lauren will reschedule you. Many issues can be handled over the phone, so we can always arrange a phone-visit between you and your doctor. In addition, no patients will be given an appointment without providing a brief reason for the visit. This helps us from being surprised by someone’s symptoms. Please do not “back-door” us and say you are coming in for a benign reason when really you have respiratory symptoms that should be handled as stated above. When in doubt, call the office and we will triage you appropriately.
The key points of the triage system we have put in place to keep everyone safe are as follows:
• If you have mild, isolated, upper respiratory symptoms (runny nose, nasal congestion, post-nasal drip, sore throat), but NO fever or cough, and have NOTbeen in close contact (within 6ft for at least 15 minutes) with someone diagnosed with COVID-19, nor recently returned from travel to a high transmission country (China, Iran, Italy, South Korea and Japan) or the Northwest US, we will recommend home care and that you not come in for an in-person visit. You are always welcome to schedule a phone visit with Dr. Mancini or Dr. Gold to talk through things.
• If you have lower respiratory symptoms (deep cough or shortness of breath) and/or fever your physician will recommend a telephone visit to ascertain if an in-person visit is warranted.
• If we determine that you need an in-person visit, the visit will occur in your vehicle in the parking lot of our clinic so as to prevent potential spread and exposure to others in the office. While this is not how we usually do things, it’s the most effective way to prevent the spread in the clinic.
• If you have severe symptoms, we will likely refer you directly to a hospital.
• Currently, we do not have the COVID-19 test kits in our office. All testing as of today is still being done through the Mass Department of Health. We are working with our lab vendor to confirm the exact specifics of when commercial testing will be available. When testing becomes more readily available we will continue to work with the Mass Department of Health and the CDC to determine who needs testing. We will not be recommending testing for just anyone with symptoms of respiratory infection; we will make this decision on a case-by-case basis using sound medical evidence and our clinical judgement.
I cannot be more explicit than this: if our staff comes into contact with someone who is symptomatic and positive for COVID-19, we may be required to be in quarantine for 14 days. As we are a small office, this may lead to a situation where we will have to close for all in-person interactions for up to (and potentially longer than) a 14-day period. If this were to occur, we would attempt to still offer telephone triage and telemedicine visits.
We are taking an abundance of caution by putting these guidelines in place to prevent the spread of this illness to the most vulnerable around us. We appreciate your understanding, patience, and effort to keep everyone in the community healthy as we all see our routines upended a bit by this virus.
Don’t hesitate to ask questions or reach out.
Carmela Mancini, DO and Jeffrey Gold, MD
For additional information please visit:
https://www.cdc.gov/coronavirus/2019-ncov/index.html
https://www.mass.gov/resource/information-on-the-outbreak-of-coronavirus-disease-2019-covid-19
Updated Testing Guidelines for More Information
Our Unhealthy Addiction to Health Insurance

Whenever I give a talk about healthcare, I ask the audience, “What is the worst addiction problem we have in the United States?”
The answers are typically the same and all are good guesses – alcohol, tobacco, opiates, and sugar are most frequently cited. I agree these are all terrible addictions that need to be addressed but, in my opinion, the worst addiction in America right now is to health insurance.
That answer usually draws a stunned or shocked silence from the audience but the numbers bear it out. The chart below shows the staggering costs American spent on healthcare in 2017. Please remember, these figures are in billions of dollars, so $2,961 spent on “personal health care” represents $2.9 trillion(!).
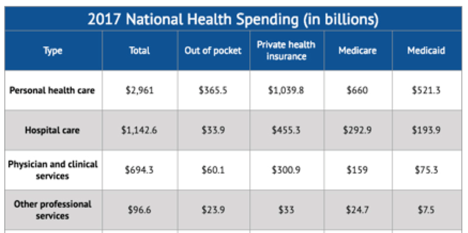
What is most shocking about these numbers is not just the high spend but the lack of value delivered in return. As a primary care physician who has practiced within the insurance-based system and now outside of it, I can tell you Americans are paying Porsche prices for Yugo performance.
The typical American experience in seeking healthcare is not good. There are often long waiting times for appointments (usually which could have been cleared up in an email or phone call), brief interactions with an actual doctor, high co-pays and deductibles, long waits at the office, a crushing amount of paperwork, and a stunning lack of communication. Does this fit into a description of “Porsche value”— especially when one gets the mystery, indecipherable bill for services weeks later?
The main mistake that we have succumbed to as a society is that we have deviated from the original intent of health insurance. The true purpose of health insurance was to protect people against financial ruin in the event of an unexpected, major occurrence – just like car insurance, life insurance, and homeowner’s insurance. But things got murky when people were indoctrinated into the belief that good health insurance should “cover everything” because “everything in healthcare is expensive.”
The irony is that, because of this mistake the “insurance” has become more expensive to the point it is unaffordable to many, and even those that can afford the premiums struggle to put money aside to cover the huge deductibles and coinsurance. Read yesterday’s article from Bloomberg Employer Based Health Insurance Costs over $20,000
The system got messed up when health insurance stopped being a form of insurance and instead became a default payment system. The dialogue below is an actual discussion I had this past year with a patient about lab tests.
Me: “Those lab tests will be 20 dollars cash through our pricing.”
Patient: “What will it be if I bill through insurance?”
Me: “We can send it to a hospital who will bill insurance but if you are on a high deductible plan I have no idea what your out of pocket will be, but I can guarantee it will be more than 20 dollars.”
Patient: “Ok, well let’s use insurance.”
Me: “You do understand part of the reason insurance is so expensive is because we use it as a payment model rather than insurance?”
Patient: “Well I pay a lot for my insurance so I want to use it.”
Me: *HEAD EXPLODES!!!*
(FYI- labs ended up being around 400 through insurance due to deductible)
The definition of addiction is “a psychological and physical inability to stop consuming a chemical, drug, activity, or substance, even though it is causing psychological and physical harm.” It’s discussions like these that make me assert that we are addicted to health insurance. This patient simply could not imagine not using their insurance for a simple procedure and, in so doing, drove up the prices unnecessarily for everyone. By doing this, we as a society, have let this addiction consume us, our paychecks, and our savings for our children and grandchildren. And we keep doing it because our brains tell us there is no other way.
The chart below illustrates the spiraling costs of our health insurance as payment system addiction:
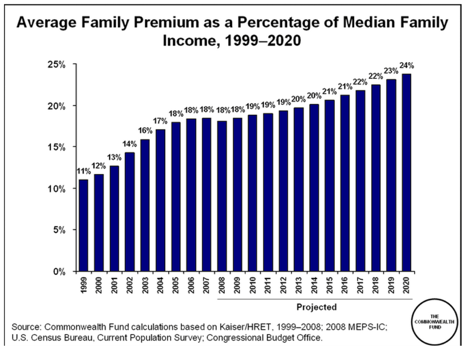
One of the health insurance benefits experts I work with is correct when he says “Today’s claim is tomorrow’s premium, copay or deductible.”
Unfortunately, the hardest part of treating addiction to any substance or belief is that denial is a major part of the disease. In order to fully treat addiction successfully, the addict has to accept that they are an addict and want to get better. Once that happens you just have to ask for help and there are resources available.
This country needs help as 20% of our GDP is on health insurance and the costs of care. It is up to us as a society to fix this as we are all patients and deserve better. We deserve high quality care when we are suffering from an insurable event and should be protected from financial ruin in such cases. We also deserve transparent pricing and quality assurance.
Above all, we deserve a system with a working payment system and to stop using insurance beyond its intended purpose. Simply stated, we must break our unhealthy addiction to health insurance. I am starting a support group called AHIAA- American Health Insurance Addicts Anonymous (ironically HIAA is already being used by you guessed it….Health Insurers Association of America). As the founding member, I am willing to admit that I too am a health insurance addict, but am now in recovery. The process of recovery has not been easy, but it has been the most rewarding process of my life. This group is established to help you through this process so please join me so we can let the healing begin.
September is National Suicide Month
 September is National Suicide Awareness Month. This is a pretty toughened lengthy post for me to write but I think it’s an important and I hope you take the time to read it. So here it goes:
September is National Suicide Awareness Month. This is a pretty toughened lengthy post for me to write but I think it’s an important and I hope you take the time to read it. So here it goes:
The video in the link below is a great message from the wife and sister of Chester Bennington- lead singer of Linkin Park- who passed away last year from suicide. It is a pretty powerful video whether you like the band or not. Although we have gotten much better as a society, there is still an unfortunate stigma and judgment around mental illness, particularly around suicide. We always hear the “how could he/she do that to their family? they were so successful and had everything? Money. Fame. Talent. etc etc. So selfish” These questions are exact proof that our understanding of mental health is poor. Although there are options for treatment and support, the access to these options leaves much to be desired- whether it be shortage of therapists, psychiatrists, or poor access to meds.
I had a case that helped me understand mental health so much better than anything I learned in medical training. He has given me permission to tell his story. He was a 20 something year old male that had just graduated college and was contemplating going to grad school. He was living at home with his parents and working while applying to grad school. He was educated, outgoing, caring and did not come from a “broken, unloving household” etc. He had suffered some significant losses in his life prior to this but always just kept plugging along not realizing that he had been depressed for years. He was just very good at hiding it from close friends and compartmentalized it very well. That is until the dam broke in his 20’s and the terrible symptoms and thoughts that go along with this illness reared their ugly head. He told me he tried to reach out to therapists/psychiatrists on his own but no one could see him for weeks and most were cash only which at the time he could not afford since he was trying to keep this from his family out of shame and embarrassment. So much for easy access. The process to find help alone was enough to increase the depression and make the thoughts worse. Shouldn’t getting help be easier? Especially when it is for a condition that it’s hard enough to admit you need help? And maybe that one moment could be what saves the person?
So the help came when his parents found him at home after leaving work early because the depression and anxiety were at an all-time high. He figured his parents would be at work midday but that wasn’t the case. It is a good thing they were home because he was brought to his primary care doctor- yes I believe that mental health care starts with good primary care- and he was referred to a therapist who saw him immediately. Things got better, but over the years therapy became a must and medication became a must as the disease would rear its ugly head many more times over. Was there trial and error with meds and luck finding the right fit for a therapist? Of course. It took work, patience, help, and understanding that this is a disease. Sometimes it is a day to day battle, but a majority of the time there is happiness now thanks to medication and help. Yet it still requires a lot of maintenance and self awareness.
So if you have never experienced mental illness in yourself or your loved ones, I hope you take from this that this disease often lives in hiding….in secrecy. It can live behind a visage of smiles and happiness and laughs. It can live behind anyone at any given time. It can present as isolation, irritability, sadness, anger, etc. There is no blood test or scan that makes the diagnosis. As Chesters sister says in the video the key is to bring this issue out of the shadows and into the light. So that’s what I thought I should do.
The patient is me and it is my story, but the illness doesn’t own me. I own it. Physicians, along with veterinarians, have the highest suicide rate of any profession in the country right now. Many of patients know this because I have spoken to them about it in privacy when they are struggling. I have been there and lived it. I have felt hopeless, ashamed, embarrassed, scared, anxious, guilty, etc. However, for a long time now I have felt happy, secure, unashamed, calm(er), and most importantly…alive to experience the love of my two children and so much other joy. Please do not crap on meds and or therapy. They can save peoples lives…or their doctors 🙂
If you are a colleague and feel you need help do not ever hesitate to reach out to me. Same goes for any other human being that reads this. Thanks for reading and know that there are people out there that get it and really do want to help, especially a local primary care doc 🙂 Thanks to Delicia M Haynes for giving me the courage to put this out there. You are an inspiration in many ways.I now hope I can do the same for others. We all have “mental health” and we need to take care of it every day. Without it, physical health means nothing. This one of my favorite Linkin Park songs. So sad that he wrote these words years ago.
Leave Out All the Rest by Linkin Park
https://nowthisnews.com/videos/news/family-of-linkin-parks-chester-bennington-on-mental-health
Seems That Amazon Likes DPC.

This article by Lydia Ramsey was published in todays Business Insider- Employers Could Use Direct Primary Care – and features our friends and colleagues Dr. Vance Lassey from Holton Direct Care in Holton KS as well as Dr. Kim Corba from Green Hills Direct Family Care in Allentown PA. The article discusses how the big three of Jeff Bezos from Amazon, Warren Buffett from Berkshire Hathaway, and Jamie Dimon from JPMorgan have announced that they are trying to fix our healthcare system Amazon, Berkshire Hathaway and JPMorgan Team Up to Try to Disrupt Health Care and they seem to be looking at using Direct Primary Care to build a solid foundation of affordable primary care for their employees. All of those questions from skeptics that I have been repeatedly asked over the past three years such as “why don’t you take insurance?”, “why should I pay twice for healthcare?” “why should I self-fund?” etc etc. are now being answered by people that have a lot more money and clout than I do. My hope is that maybe now people will not only start following, but also start teaming with a group of renegade primary care doctors across the country that have been doing this model for the last decade because they had enough of the “healthcare cartel.” If you use Amazon maybe you should also consider using a DPC doc.
An Uproar in the Land of the GIC

I know it has been a while since I have written anything, but it has been a bit since I have seen something that has really driven me to write about. Yesterday I happened to see an article that was in the Boston Business Journal regarding health insurance options for our state employees that are on GIC plans- police, fire, DPW, teachers, etc. The following is a link to a free version by Martha Bebinger at WBUR Major Mass. Insurers Dropped From State Employee Health System. The three major players that are now out are Tufts, Harvard Pilgrim, and Fallon. What I find interesting about this change is that the GIC is quoted in the article are saying that “moving members to a more limited, less expensive number of insurance plans will save the state $20.8 million in the next fiscal year with little disruption.” I am very curious to see what these premiums will look like to our valued state employees. As a self-employed business owner I had to do my renewal by January 1st and by choosing Tufts Direct I was not only able to have great hospitals like Lahey and Tufts Medical Center in the network, but also saved $400 a month in premium compared to a similarly structured plan (i.e. same deductibles etc) with Neighborhood Health Plan that is owned by Partners. So again, I am curious to see where the costs savings will be? I highly doubt it will be to the employees.
See the issue here is that no one is actually addressing the cost of health”care” and only focusing on the cost of insuring it. The public has been led to believe that everything in “healthcare” is so expensive that we need a prepaid “insurance card”- one with a very large finance charge while we are at it- so we don’t go broke. The irony is that it is the actual cost of insuring everything under the sun that is making people go broke. So employers- including the state government- have only two options to keep their spend under control: 1. transfer more cost to employees by raising out of pockets such as deductibles/copays/coinsurance and 2. limiting the network of hospitals/doctors employees can use with restrictive HMO-type plans. (As already mentioned, given that one of the options left here is NHP is quite strange given that Partners hospitals/practices are much more expensive but let us wait and see what the premiums are.) As a result of union leaders not wanting to see their employees carry huge out of pocket responsibilities such as deductibles and the like, what other options does the state have? When you expect a third party to cover 90-95% of your care this is what will happen. You lose money and the freedom to choose.
So my question to all GIC beneficiaries is do you really think your employer and the insurance carriers they are choosing are going to help address this cost equation for YOU? Are they providing the actual care you receive? No they are not , but they are determining where you can and can not get it from. So speak up! I lost a lot of you as valued patients when I stopped taking your “payment/insurance card” and instead wanted to be paid directly by you for all your primary care at a reasonable monthly fee that averages out to $75 a month. Sadly what you did not see is how on your side I was and continue to be. Your choices of payment cards are now fewer and fewer and my educated guess is that it will cost you more to carry the card(s) offered to you and fewer places where you can actually use them. So why not grab your local DPC doctor as an ally so that we can fight this fight together and get more options for you- like say a higher deductible plan that works like real insurance by covering major expensive medical care not the affordable part like primary care (lower premium) and combine it with a Direct Primary Care option. The only way we fix this system and the cost to you and the taxpayers of Massachusetts is to disrupt it from the ground up instead of letting policymakers do it for you from the top down. If you need more proof or evidence that it works look at what my colleague Dr. Rushika Fernandopulle has done at Iora Health in Boston for GIC members on Unicare: Iora Health and GIC Combine to Offer DPC to Unicare Enrollees. Why doesn’t NHP, Tufts, and HPHC offer the same? Hmmm. Also look at what Union County in North Carolina has saved offering DPC to their county employees! And this is with only 40% enrolled in the high decutible/DPC plan! Direct Care Helping North Carolina Public Sector Save Big On Health Care Claims. If you’re really bored but truly want to see how this worked in North Carolina watch this video. It includes my fellow DPC colleague and friend Dr Amy Walsh. It may be an hour but it is well worth it in my opinion.
I am willing to speak with any town administrator, union leader, state official you would like. Just ask them to schedule a meeting. You, that provide our communities with so much service, deserve much much more when it comes to your coverage and your care. Remember, they are usually not the same. Thanks for listening.
A Leap of Truth

This is dedicated to all of those on the precipice of choosing between your norm versus your actual truth. Not who you project but who you are when no one else is looking.
People often use the term “Leap of Faith” in their motivational language. Wikipedia defines a leap of faith as “an act of believing in or attempting something whose existence or outcome cannot be proved.”
Well I would like to coin a new term- a Leap of Truth. This is an act of believing in or attempting something whose existence or outcome can be or may already be proven, but one is too damn scared to admit it and step toward it. People often ask me what led me to take such a huge risk by leaving a very well paying job as a primary care physician working for one of the “best” hospital systems in the country. The answer is very simple- I took a leap of truth. I knew from the moment I filled out a coding/billing form in my residency clinic after seeing ten patients in one half-day session that this type of primary care medicine was not going to be my truth. For nine to ten years or so I struggled to put my truth into words- never mind being close to putting it into action. I could not even define it…yet. I just knew that 10 minute visit, impersonal assembly line medicine was not going to fit in the definition. I knew that spending a majority of my day trying to prove my worth to some 3rd party insurer or government agency was not going to be part of it either. I just wanted to do what I dedicated my education and life to- taking care of my patients to the best of my ability. Everything else was just useless.
So one winter night in December 2013 I was sitting on my iPad trying to figure out Twitter. After being on there for ten minutes or so, someone I followed retweeted a tweet from Dr. Josh Umbehr at AtlasMD in Wichita KS. It read something like this: “Imitrex injection for migraines 200 and something dollars in local ER. $9.10 in our clinic. #DPC” So I said to myself “what the hell is DPC and why I have I never heard of it?” Within 5 minutes I hit reply all and asked exactly that. Within minutes Josh messaged back and said he would be happy to set up a call so that I could learn more. So that next night I sat on a call with him and realized I was getting closer to defining my truth. My truth was and is Direct Primary Care. After researching the model and the labyrinth that we call American health policy for almost a year, I knew that I had to leave my norm and take a Leap of Truth.
Of course I had a lot of doubters, naysayers, skeptics and flat-out demoralizers tell me I was going to fail. Some of my favorites were “This isn’t Kansas…this is Massachusetts” and “This will never work in Massachusetts.” My all time favorite was when i told an elderly patient- one who had just switched to me after his prior doctor of 20 or so years had retired- that I too was leaving. As an employed doctor I was not allowed to do this, but I felt that it was the appropriate and right thing to tell him given his age and uncertainty in regards to his future care. So I explained the model of DPC and told him he was more than welcome to come with me if he so desired. His response upon learning I wanted to work for cash rather than government/insurers was “what are you some kind of greedy Jew or something?” You can not make this stuff up. My response was with a chuckle as I said “yeah I guess if you believe taking the biggest professional risk of my life and putting myself into a mountain of debt to do it defines a greedy Jew, then yeah I am a greedy Jew through and through and proud of it.” Needless to say, but this kind gentleman among many others did not come with me to my new practice. However, I persisted walking through the mire because I knew in my heart it was the right thing, regardless of what others had to say.
Those months from April of 2014 to December 2014 were some of the hardest months of my life. I was basically working two jobs. I was seeing a full load of patients act my old job and meanwhile trying to build a new practice. God only knows what my blood pressure was during those months, but I look back with not one regret. Sometimes doing the right thing is just really freakin hard, but once you find your truth you will find that there is nothing more comfortable….not even the norm you have grown so accustomed to.
My favorite television show of all time is Lost. Yes, some people hated it and some people loved it, but few were in between. The irony of this is that the whole series was really about the “in-between”- science vs faith, reality vs destiny, life vs death. It wasn’t about polar bears being on a tropical island. I have attached a video clip that shows the ongoing debate on the show between Jack Shephard as a man of science and John Locke as a man of faith. (Sorry for the length and ad that pops up in the middle.) So I guess the message here is that there is something between faith and science and between life and death, but it does not have to be a painful purgatory. It can be a truth in which you find peace. Do not settle for being a slave or pawn to the “system”. You put yourself through college, medical school, residency, debt, etc etc. When you think about the doctor you are vs the doctor you hoped to be you may realize that the truth is somewhere in the middle. So stop looking at DPC or some other career change as a Leap of Faith, but look at it rather as a Leap of Truth- your truth and only yours. No one can take that away from you no matter how hard they may try.
To Teach Is To Learn
Last week I was notified of an incredible honor. I received a citation of excellence in teaching along with 11 other clinical faculty in Family Medicine by the Tufts University School of Medicine 3rd year students. I am pretty sure this recognition does not come with a check, a free car, or a safari adventure but it means a heck of a lot more to me than any of those items. I would not be a physician today without the many incredible teachers I have had- from kindergarten through high school, college, medical school, residency, and clinical practice. There have been a few duds along the way, and not because they were not knowledgable, but moreso because they just seemed disengaged and unhappy teaching. Sadly a few of these duds were in medical school and unfortunately they had no idea the negative influence they had on me. One of them actually drove me away from the field of medicine that I was originally interested in pursuing. So I promised myself back then that I would never treat students that way if I ever had the opportunity to teach. I have only strived to have a positive influence on my students regardless of the field of medicine they choose. And now, by exposing them to Direct Primary Care, I hope they might realize that there is a future in primary care besides the current option of being an employed physician. However , what I did not realize when I first started teaching about ten years ago, was the incredible influence they would have on me.
Over the years, my students have reminded me of why I chose to pursue a career in medicine in the first place- particularly primary care. I see their thirst for knowledge, their drive to try to know everything, their passion to care for people, and their desire to impress me. I often chuckle on the inside when I give them a project or something to look up and they think its just a routine assignment I have given them, when in reality, it is solely so I can learn a new topic/disease or relearn an old topic/disease I have not seen in years. They keep me on my toes and challenge me to be a better educator, doctor, and person in general. They make me realize how under-appreciated primary care is as 6 week rotations do not even scratch the surface of the knowledge base that is needed to do this job well. One of the joys of medicine is that every day is a learning experience, and my students just enhance it and make it that much more enjoyable.
So, as my children finish 1st grade today (with perfect report cards I may add) I thought it would be apropos to write something that shows my appreciation for all the teachers out there, and for the students that remind us teachers that we too are still all students.
PS. Thank you to Tufts Medical School for allowing me to teach and for this incredible honor.
While Congress Fiddles, Patients Lose Patience

Published in the Boston Business Journal April 7, 2017:
The longer Republicans debate and dissect the Affordable Care Act, the more people are turning to Direct Primary Care (DPC) physicians. Unlike the recently proposed American Health Care Act — and the Affordable Care Act it is seeking to replace — direct primary care is both affordable and easy to understand.
The rising popularity of DPC practices in Massachusetts and in more than half the states where it is being practiced is in stark contrast to the utter confusion and fear that has ensued since Congress and White House set out to repeal Obamacare. A health care system once focused on prevention has given way to expensive intervention and specialty care. Experts disagree on how to fix our health care system, but it is well understood that what has been driving up the cost of health care are prescription drugs, overutilization of our hospital emergency rooms for non-emergency primary care, escalating prices for medical procedures, and unnecessary diagnostic tests. What patients — and doctors — need from our health care system is simplicity. Think of how we use car insurance to protect us from personal injury and car damage — not for the replacement of tires or windshield-wiper blades. We shouldn’t use health insurance for routine primary care.
Rebuilding the primary care foundation of our health care system won’t fix all of what is ailing health care, but it would reset a system that now largely benefits the insurance industry and pharmaceutical companies. A study by the health policy journal Health Affairs found that a direct primary care practice they studied was nearly half the cost to the patient when they purchased a lower-premium, higher-deductible insurance plan. A 53-year-old man who would have paid $11,068 for a one-year $1,000 deductible plan instead bought a higher-deductible plan and cut his health care costs by more than $4,000 annually — and he actually spent more time with his physician.
During the course of an appointment that is typically an hour or longer, DPC physicians can figure out why a patient hasn’t been sleeping rather than just writing them a prescription and dashing off to the next 12- minute appointment. We get to know our patients, their diet, whether they are exercising. That consultative relationship is critical to prevention of future and expensive illnesses such as heart disease, cancer and diabetes. Direct primary care physicians aren’t necessarily better doctors — we just spend the time that it takes to be a good doctor and actually listen to our patients. But you can’t fix what you don’t have the time to see or hear.
DPC, The Netflix of Healthcare
When is the last time you went to a Blockbuster Video store on a Friday night to peruse the shelves for a rental? Yup, almost ten years ago. The key question is why is it extinct? There are many obvious reasons- inconvenience of having to go search the shelves, finding out the movie you want is out, and the most obvious is innovative disruption by companies like Netflix and Amazon (see article from Forbes below).
The key component of the decline of Blockbuster Video/On Demand and the rise of Netflix is what network scientists refer to as the “threshold model of collective behavior.” In other words, this is how innovation takes hold and finds success in society whereas other products/concepts fail and drift away because they do not keep up and change to meet the needs of the consumers of the service. Blockbuster tried to adapt but it was too late. It dropped its late fees- which was their key to profitability- and spent approximately 400 million dollars instead. All the while Netflix was charging an affordable monthly fee, could deliver DVD’s to your door, and figured out how to stream content. And even though their library was not as extensive, their affordability and no hassle service made them what they are today.
So what in gods name does this have to do with me? Well, I think it is pretty obvious. The Direct Primary Care model is the Netflix of Medicine. You pay less than a coffee a day, or less than an average cable/cell phone bill a month, so that you can receive primary medical care the way it was and should be delivered. It is easy, accessible, transparent, dependable, and personalized. We bring care to you not vice versa. There may be a month when you stream ten different TV shows or movies (not speaking for myself of course) or there may be a month when you watch none, but Netflix is always there. DPC is the same, and more importantly, there is a personal relationship and level of trust that is built to help you stay healthy, be accessible when you’re sick and need care, and more importantly help guide you through the tangled web of the US Healthcare/Insurance system.
The current system of insurance-based primary care requires in person visits for all care in order to bill your insurance – even for matters that could be handled remotely with a quick phone call, text message, or Skype session. This same in person care requires copays/deductibles for each visit, provides a maximum of 10-15 minutes with your doctor on a good day, and is inflexible to scheduling around your personal life. Also, with more and more people on high deductible health plans cost is being shifted onto patients. How do you shop for elective, outpatient care like labs and imaging studies in a system of zero transparency? How, in a country as developed and wealthy as ours, did it take this long to apply simple, affordable innovation to the most important, yet most costly, consumer-based product we have- our health and well-being. The current model of insurance-based primary care is Blockbuster video. Where do you want to be when it goes bankrupt?
Endnote: it is well worth an hour of your time to watch this incredible lecture by David Goldhill- CEO of the Game Show Network and author of “Catastrophic Care- How the American Healthcare System Killed My Father”- that I was fortunate enough to be present at this October in Dallas. His book is also worth the read. Besides a mortgage, healthcare is the largest expenditure we have so be informed and learn.
If you want to learn more in depth details about the decline of Blockbuster, please read this great article from Forbes A Look at Why Blockbuster Failed

